Learning and improvement in practice: UHB Learning and Improvement Summit joint panel session
At University Hospitals Birmingham NHS Foundation Trust’s Learning and Improvement Summit on the 22nd April, colleagues from University Hospitals Birmingham NHS Trust, Bristol NHS Group (including North Bristol NHS Trust) and Radar Healthcare shared practical examples of how a modern Quality Management System can bring fragmented data together, simplify governance, and turn safety, experience and workforce intelligence into learning and improvement.
From data to insight: turning governance information into learning
Opening the discussion, Justin King, Director of Clinical Services at University Hospitals of Birmingham NHS Trust, highlighted the scale and complexity of modern governance. Organisations are managing tens of thousands of incidents each year alongside risks, complaints and other datasets, much of it qualitative in narrative.
The question posed to the room was simple:
how do we use what we already collect to drive meaningful change?
Paul Cresswell and Jenny Booth from Bristol NHS Group and North Bristol NHS Trust reinforced a consistent message: the biggest gains come from getting the foundations right. Start with clear, workable processes and high-quality data then build dashboards, analytics and AI on top. Bringing information together from databases, spreadsheets and standalone systems, they emphasised standardising how governance work is done so insight is trusted, repeatable and easier to act on.
Flexibility came through strongly. Acute care doesn’t always fit neat workflows or fixed responsibilities, so digitisation has to support real-world complexity. For Jenny and Paul, the work with Radar Healthcare focused on bringing governance into one place while still allowing teams to operate at pace, without forcing frontline staff into processes that don’t reflect how care is delivered.
North Bristol NHS Trust: making audits easier and more meaningful
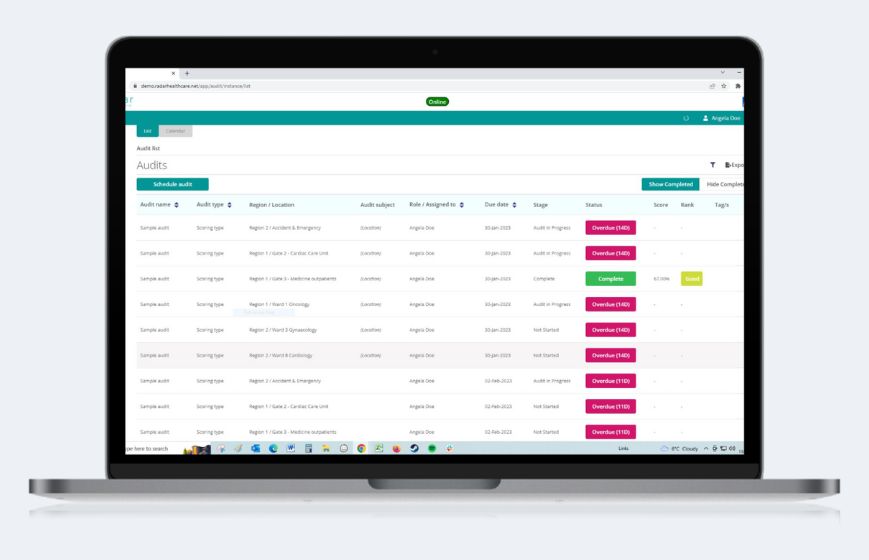
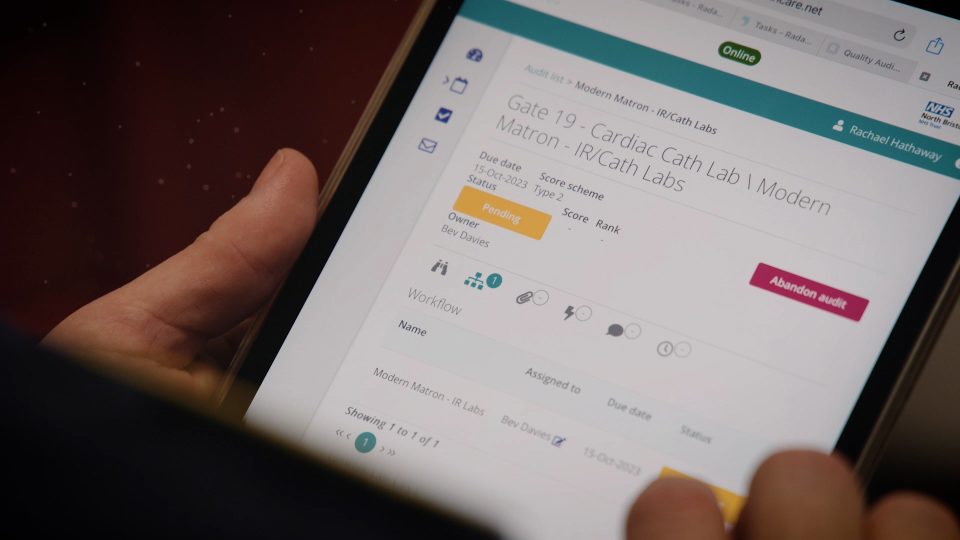
Jenny described how, in 2022, the audit experience wasn’t working for staff: completion rates were low, the process felt time-consuming, and teams couldn’t progress to the “so what?”. The redesign made each question clearer, removed what wasn’t needed and made audits easier to complete at the point of care, for example, using simple iPad-based workflows rather than searching for a computer.
Jenny described the impact as both cultural and practical: teams could see their own performance more clearly, leaders could track completion instantly, and ownership of actions by team/area became more explicit. Audit completion increased to around 90–95%, with sustained monthly delivery since launch over two years ago. Crucially, time spent manually manipulating spreadsheets reduced substantially, releasing 4–5 days each month for a clinical quality lead to focus on monitoring, insight and improvement rather than data collation.
University Hospitals Birmingham NHS Trust: aligning governance, insight and clinical strategy
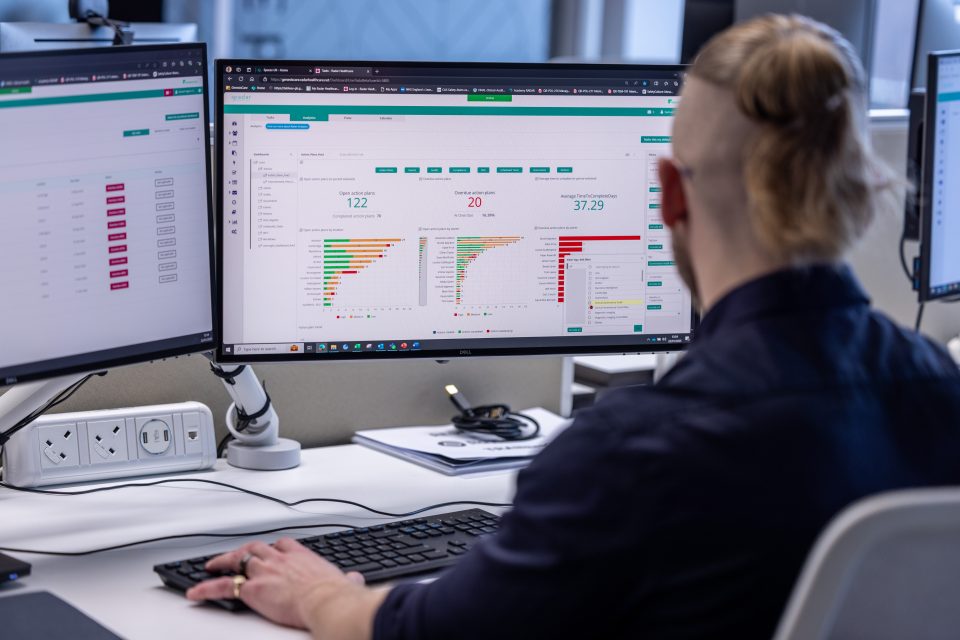
Abraar Mirza, Radar Manager at University Hospitals Birmingham NHS Trust, emphasised aligning governance activity to clinical strategy, using the QMS, data and insight to make governance meaningful for services and specialties, and to support decision-making that matters. The ambition shared was clear: reduce time spent manipulating spreadsheets and increase time spent interpreting signals, prioritising action and supporting continuous improvement.
Abraar also shared early experimentation with AI-enabled support for recurring analysis requests, for example, quickly checking whether a theme appears to be increasing or decreasing and producing a consistent summary. By connecting adjacent datasets, the team described being able to create richer multi-process extracts and use that analysis to refresh trust safety priorities. One important reflection was that better detection can surface more issues than an organisation has capacity to address, so prioritisation remains essential.
Radar Healthcare: partnership, onboarding and responsible innovation
Rhian Bulmer reflected on a partnership-led approach focused on continuous feedback from trusts. This shapes product development, onboarding and configuration in real-world settings.
There isn’t one standard NHS process model. Peer learning and communities of practice play an important role in helping organisations share what works and adapt workflows to local needs.
The focus remains on supporting organisations to build strong foundations, while continuing to evolve capabilities such as AI in a controlled and meaningful way.
Key takeaways for quality and governance teams
-
Start with the work
Map real clinical and governance workflows, then simplify before adding analytics or automation.
-
Design for the frontline
fast, mobile-friendly, low-duplication journeys are what make governance activity routine.
-
Make insight actionable
reporting should show what needs attention, who owns it and what improvement activity is in motion.
-
See cumulative risk earlier
joined-up datasets can reveal patterns that individual wards and teams can’t see in isolation.
-
Use AI responsibly
put governance and information controls first; focus AI on reducing administrative burden and strengthening signal detection, not replacing professional judgement.
The shared message was that building a learning organisation is as much about culture and process as it is about technology. Bringing governance activity into one coherent system can free up time, strengthen accountability and improve visibility but the biggest gains come when insight is linked to clear improvement priorities, and teams keep iterating based on what the data is telling them.
Audience FAQs
AI agents as an early warning system
An audience member asked whether AI agents could help move governance beyond retrospective dashboards, surfacing live “early warning” signals by combining multiple inputs (e.g., incidents, complaints, patient experience and staff survey feedback) and prompting timely leadership intervention before risks escalate.
The panel broadly agreed with the direction of travel, while emphasising safeguards. Rhian Bulmer from Radar Healthcare described ongoing work with partner trusts and roadmap development towards more predictive capability, supported by tight controls to reduce noise and keep outputs useful. Paul Cresswell from Bristol NHS Group highlighted complaints as a practical near-term candidate for AI support: using automation to identify key narratives and themes, and to support drafting, while maintaining strong information governance and ensuring relationship-based work (such as rebuilding trust with complainants) remains human-led.
Justin King from UHB noted that some benefits are already being realised at small scale: tasks that previously took half a day, such as extracting and reading incident narratives to test an emerging trend, can now be completed in minutes.
2) Workforce assurance: correlating staffing, skill mix and care red flags
A Director of Nursing asked how to link workforce assurance with quality “red flags” in a way that stands up to scrutiny. The challenge raised was that roster and vacancy dashboards can show shifts are filled, but not whether the right capabilities were present (novice vs expert mix, training status, where staff time was spent), nor how that reality correlates with harm events such as falls, tissue viability incidents or infection prevention and control concerns.
Rhian Bulmer from Radar Healthcare responded by outlining how, in principle, linking staffing datasets (skill mix, acuity, agency use and related indicators) with incidents, patient feedback and other quality signals can create a stronger, evidence-led “go and see” prompt. She noted this typically follows the foundations of rollout and data quality and may involve integrations or partnerships so workforce information can be analysed alongside quality governance information in one view, supporting earlier intervention and clearer scrutiny.