Why care home groups need more than a care planning tool
Ask a Director of Quality at a multi-site care group what keeps them up at night and the answer is rarely about the quality of care being delivered. The teams on the ground are skilled, committed and well-supported. The care planning is thorough. The daily records are detailed.
What tends to keep the Director of Quality awake is a different kind of question:
what is happening across all twenty sites, right now, and can I show it to the board on Friday?
For most multi-site care groups, the honest answer is not straightforward. And the reason usually has nothing to do with how well the organisation is run.
Care planning tools do exactly what they were designed to do
The UK social care sector has made genuine progress in digital care planning over the last decade. Most multi-site care groups now use a dedicated care planning platform — a system that records assessments, care plans, daily notes and medication management at the level of the individual resident. The best of these platforms are excellent.
The key phrase here is ‘at the level of the individual resident.’ Care planning platforms were designed to support the relationship between a care worker and the person in their care. What they were not designed to do is give a Group Director a real-time view of governance, risk and compliance across all locations. That is a different function entirely.
And one that most multi-site care groups are currently managing without the right infrastructure.
The governance gap that opens as care groups scale
When a care group is running two or three sites, the Director of Quality can reasonably maintain an overview through regular visits, phone calls and familiarity with each location. Governance is a manageable, largely manual process.
At ten sites, that approach starts to strain. At twenty or more, it breaks. The volume of information, the number of variables and the pace of change across all locations exceeds what any individual or small team can monitor without the right tools in place.
Invisible trends
Incident patterns visible within a single site but invisible across the group until someone manually aggregates the data.
Masked variation
Audit completion rates that look acceptable on average but hide significant variation between individual locations.
Lost actions
Investigation recommendations tracked — if at all — in email threads that nobody outside the immediate team can see.

“If those incidents had been written on paper and put in an in-tray, we would have missed it. The system showed us what a person couldn’t tell us.”

“Prior to Radar Healthcare, we were operating eight systems with lots of information that were not really talking to one another, which took valuable time. Radar Healthcare has given us the means to see the bigger picture, connecting the dots for us internally and making our operations more efficient.”

“Radar Healthcare has helped us be Outstanding! It has provided visibility and central governance around all areas of quality and compliance, enabling us to triangulate data to identify key themes and trends. Five out of our six CQC regulated services are now rated Outstanding in the well-led category.”
“Radar Healthcare has replaced all our Manager Workbooks. Instead of manual spreadsheets, we’re able to customise workflows to capture exactly what we need and use dashboards for oversight, so our Area Managers are saving on average two days a month.”
What CQC expects from multi-site care groups
CQC’s Well-Led domain is explicit about what good governance looks like at group level. Inspectors are not simply asking whether processes exist at each site. They are asking whether group leadership has the information they need to manage risk and drive improvement across the whole organisation — and whether they can demonstrate that governance infrastructure is working consistently, not just in the best-performing locations.
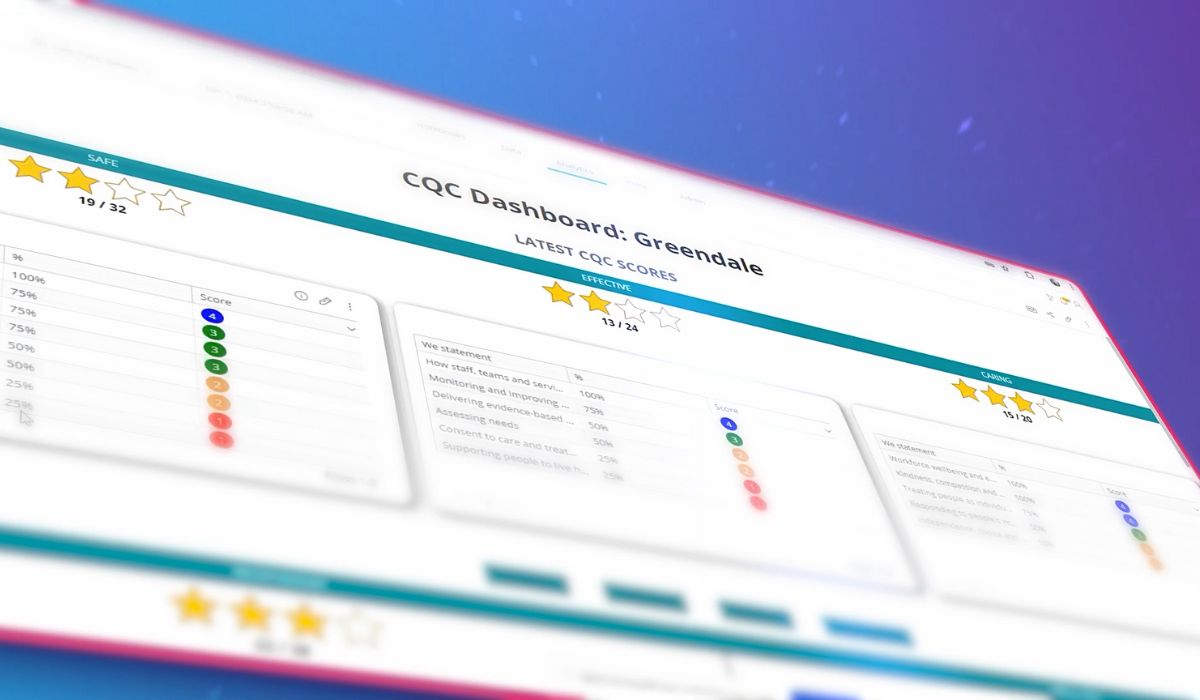
That means being able to show incident trends at group level, audit completion rates by location, evidence that actions from investigations were assigned, tracked and closed — and a coherent picture of CQC readiness across every site. Not as a manually assembled report compiled the week before an inspection. As a live, accurate view that exists all the time.
The governance layer: what it is and why it matters
The answer to the governance gap is not to replace the care planning tools that frontline teams rely on. Those tools are doing important work and disrupting them would create problems of its own. The answer is to add a governance layer above them.
 “Care planning and governance are two different functions operating at two different levels of the organisation. Care planning supports the delivery of care to individuals. Governance supports the leadership of the organisation as a whole. Both are essential. Neither replaces the other.”
“Care planning and governance are two different functions operating at two different levels of the organisation. Care planning supports the delivery of care to individuals. Governance supports the leadership of the organisation as a whole. Both are essential. Neither replaces the other.”
Rhian Bulmer, Chief Customer Officer at Radar Healthcare
The most effective multi-site care groups use both: care planning tools that support frontline teams at site level, and a governance platform that gives Directors of Quality, Regional Managers and boards the connected group-level picture above them. Radar Healthcare is built precisely on this model — working alongside the tools already in place, adding the governance layer above them that no single-site system was designed to provide.
What the connected governance picture looks like in practice
When governance is properly connected across a multi-site care group, the change is felt at every level of the organisation.
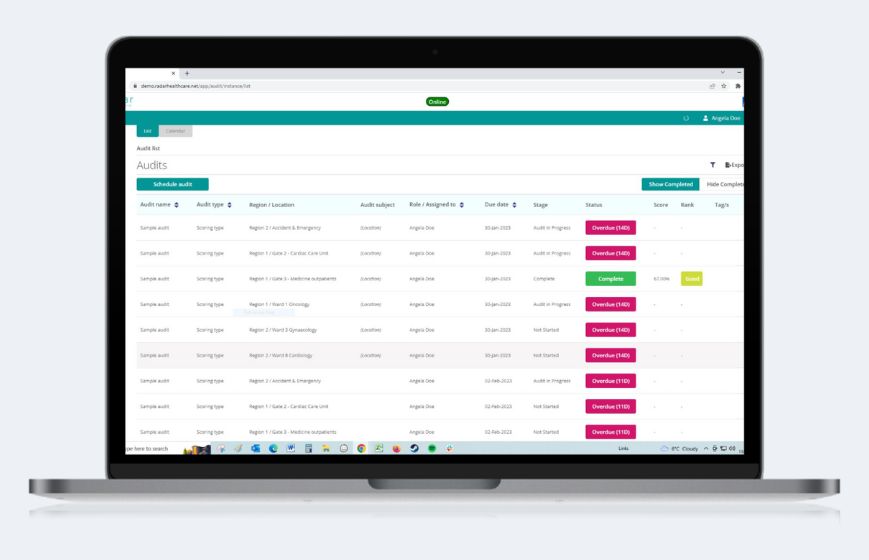
The Group Director of Quality can see incident trends across all sites in real time, with the ability to drill into individual locations when something warrants closer attention. Audit completion rates are visible by site and across the group. Open risk items are flagged by severity and location. CQC readiness is not a question that requires a week of preparation to answer.
The Regional Manager can see which sites need attention this week without waiting for a site manager’s report to arrive. The board receives reports generated from live governance data, not assembled manually the night before. The confidence that comes from that shift is tangible — in board conversations, in regulatory interactions, and in the culture of the organisation.
The starting point
For care groups considering how to strengthen their governance infrastructure, the starting point is rarely a wholesale technology replacement. The care planning tools in place are doing important work and should stay. What is needed is the layer above them.
The groups making the most meaningful progress on governance maturity are those that have made that distinction clearly — and invested in the infrastructure to give group leadership the visibility it needs to manage effectively, respond confidently to CQC, and demonstrate quality consistently to every stakeholder who asks.