Reimagining Maternity Care In The NHS
Tags:
Listening, learning, leading: The future of maternity care
Maternity care in the UK is at a defining moment. For generations, the NHS has delivered countless safe and positive birthing experiences, but today systemic pressures mean not all families receive the NHS maternity care they deserve.
Workforce shortages, outdated processes and policies, and stark disparities in outcomes are creating stress within the system, leaving pregnant women and families without the reassurance they need. NHS maternity complaints are increasing, and some families are left unsure how to make a complaint through the NHS complaints process or whether to raise their issues with a complaints team directly.
Yet at Radar Healthcare, as specialists in risk, quality, and compliance, we believe this is also a moment of profound opportunity.
By confronting these challenges with clarity and by embracing both technological innovation and compassionate leadership, we can build a maternity service that is safer, more equitable, and more responsive to women and families across the country.

A system under pressure
The financial and human cost of failings in maternity care is difficult to ignore. Since 2019, the NHS in England has faced an estimated £27.4 billion bill for maternity care failings, an amount significantly higher than its £18 billion newborn budget.
This burden is being driven by a rise in legal claims, which nearly doubled to almost 1,400 annually by 2023 (The Guardian). Families are often unsure whether to contact their local hospital, GP practice, or community services when they want to raise concerns or provide feedback about the service provided.
Even more striking, NHS Resolution anticipates £37.5 billion in future claims liabilities, a figure that underscores the urgency of transformation (The Guardian).
Many families seek confidential advice or turn to a patient advice liaison service for helpful information, but the process can feel fragmented across different NHS organisations, each NHS trust and each NHS body responsible for providing services.
In a recent popular podcast, “He Said, She Said”, co-host and influencer Louise Thompson states how she recently spoke on a panel in Parliament about her experience of birth trauma to help shape the “National Maternity Investigation” which aims to change policies to help improve maternity care (due to be released in December 2025).
The podcast also reveals that between 2023 and 2024, the NHS paid out £3billion in medical negligence claims, and 41% of those claims are related to maternity care (He Said, She Said).
Louise states: “Each year they receive a budget, and they factor in medical negligence claims. When instead, we could be working on changing some policies so that women and families are better educated and informed – so they know exactly what their options are when it comes to labour, so that they can choose, be listened to, and get the right care during the antenatal stage, in the hospital, and then when leaving the hospital with adequate postnatal care. That would save an awful lot of money.”
Alongside this financial strain is the reality of rising complaints. Over a two-year period, maternity services and midwives received more than 25,000 complaints about NHS maternity services through the NHS complaints procedure, with maternity department grievances alone rising by 16% from 3,970 in 2020–21 to 4,610 in 2021–22 (Been Let Down?). Most complaints related to communication or delays, while others involved hospital care, antenatal appointments, primary care services or gaps in social care support.
The Parliamentary and Health Service Ombudsman further highlighted that 84% of women felt healthcare professionals were not listening to them, with 65% of maternity complaints between 2020 and 2022 involving communication failures (ombudsman.org.uk).
In many cases, families contacted an independent service or their local integrated care board for further information on how to escalate concerns on their behalf, but some were left without clear contact details.
James Titcombe, chief executive of Patient Safety Watch and co-founder of Harmed Patients Alliance, recently declared in his popular blog: “Too often, families report their concerns being ignored – sometimes with tragic consequences. We must break down the cultural and organisational barriers that stop staff listening and create psychologically safe environments where speaking up is valued and acted upon” (Patient Safety First). This reflects the need for a stronger learning culture across all NHS organisations and other NHS service providers. Charities such as Maternity Action also provide crucial advice and advocacy for families navigating this complex system.
Perhaps the most sobering reality is the rise in maternal mortality. Between 2020 and 2022, the maternal death rate increased to 13.41 per 100,000 maternities, a 53% rise compared with 2017–2019 (University of Oxford).
The impact of COVID-19 and unmet maternal health needs, including gaps in mental health services, has contributed to this increase, but underlying inequalities have made the situation even more stark.
Black women are approximately 2.8 times more likely, and Asian women 1.7 times more likely, to die during or shortly after pregnancy compared with white women (MBRRACE-UK). Families facing these disparities may not know where to turn, whether to seek support from their GP surgery, ambulance service, district nursing, or even a care home or other NHS service provider. Families with previous pregnancies that had complications may also struggle to have their history recognised in future care plans.
These figures do not exist to cast blame. Rather, they are a call to action, urging the system to listen, learn, and lead with greater urgency and humanity.
Insights from CQC maternity inspections
Inspection data also reflects the complexities of today’s maternity care. Between 2022 and 2024, the Care Quality Commission (CQC) inspected 131 maternity locations, finding that 47% required improvement and 12% were inadequate. Only 4% were rated outstanding, while 48% were considered good (Care Quality Commission).
Yet when inspectors focused specifically on safety, the picture was starker: not a single service achieved an “outstanding” rating. Almost half required improvement, 18% were deemed inadequate, and only 35% were rated good.
By late 2023, approximately two-thirds of maternity units had received ratings of “requires improvement” or “inadequate,” a concerning increase from previous years (Hansard).
However, within these reports are also accounts of excellence: examples of strong leadership, collaborative culture, and effective teamwork. These pockets of best practice are not anomalies; they are proof that transformation is achievable.
Encouragingly, several NHS organisations have recently been recognised for their commitment to safe, compassionate, and well-led maternity care. These include Wirral University Teaching Hospital FT, Royal Cornwall Hospitals Trust, East Cheshire Trust, and York Teaching Hospitals FT (Health Service Journal).
Signs of progress and resilience
Yet even amidst the challenges, there are positive signs of progress that should not be overlooked. The CQC’s 2024 Maternity Survey, which gathered responses from 18,951 women, revealed that 76% were ‘definitely’ asked about their mental health, up from 75% the previous year.
Furthermore, 89% reported that they received mental health support when they needed it – an increase from 85% in 2022 (Care Quality Commission). These improvements, while incremental, matter deeply in the lived experiences of families.
Encouragingly, most respondents also felt listened to (83%), communicated with clearly (88%), and involved in decision-making (80%). Families reported being able to discuss their options in each appointment, with a greater sense of shared responsibility between patients and staff.
Information on the risks of induced labour was provided more consistently (74% in 2024 versus 69% in 2023), and partner presence after birth rose from 56% to 63% over the same period (Care Quality Commission). Better communication about screening tests and monitoring baby’s movements was also noted as an area of improvement.
As previously mentioned, at a national level, attention among health professionals and politicians is also turning to maternity care reform. In June 2025, the Health Secretary commissioned a rapid national investigation into maternity and neonatal care, co‑produced with clinicians, experts, and bereaved families. Its findings were due by December 2025 (GOV.UK).
Meanwhile, the government’s 10-Year Health Plan includes the procurement of a national virtual ward system, integrated into the NHS App and Single Patient Record (SPR), with significant potential to reshape maternity services (Health Service Journal).
The 10-Year Health Plan states: “We will undertake national procurement for a new platform available to all NHS provider organisations. This will include the ability to remotely monitor patients, with data flowing through to the NHS App and Single Patient Record – enabling proactive management of patients to become the new normal.”
It continues: “New legislation [will] place a duty on every health and care provider to make the information they record about a patient available to that patient. We will also legislate to give patients access to their SPR by default.”
“Our ambition is that from 2028, patients will be able to view it securely on the NHS App. Over time, that data will include not only medical records, but also a personalised account of health risk, drawing from lifestyle, demographic and genomic data – to help personalise the NHS’s service offer and to support individual behaviour change.”
It goes on to say: “We know from both evidence and our engagement that experiences of maternity care are not good enough, and that mothers’ preferences are frequently ignored. The SPR will ensure maternity teams have all the information they need about previous consultations, medical history and stated preferences, helping them provide genuinely high-quality, personalised care.”

The role of technology in transformation
Technology alone cannot solve every challenge, but when used thoughtfully, it can empower staff, streamline processes, and enhance safety.
For maternity care, the national Single Patient Record represents a step change.
By providing clinicians with seamless access to medical history, consultation notes, and patient preferences, the SPR offers the foundation for more personalised, safe, and compassionate care.
The national virtual ward system, integrated with the SPR, opens further possibilities. Through remote patient monitoring, maternal vital signs such as blood pressure and fetal well-being indicators like the baby’s movements can be tracked in real time, with timely alerts for deterioration. This approach could ease pressure on overstretched labour wards, high-risk clinics, and postnatal care units, allowing care teams to intervene proactively rather than reactively.
This approach could ease pressure on overstretched labour wards, high‑risk clinics, and postnatal units, allowing care teams to intervene proactively rather than reactively.
Wearable technology, when embedded within this model, could offer continuous oversight of maternal health, giving both patients and clinicians greater reassurance. For example, an obstetrician could remotely review data trends to tailor care to a woman’s individual needs and circumstances.
Additionally, generative AI tools hold promise for reducing administrative burdens. From automating documentation to analysing incident data, AI can release clinicians’ time to focus on what matters most: direct patient care.
Importantly, AI also offers the potential to identify patterns in complaints and incidents that might otherwise go unnoticed, enabling system-wide learning and faster quality improvement.
Introducing more Digital Midwives and Nurses – professionals who bring together clinical expertise and digital skills – enhances the secure management and sharing of health data, as well as implementing the right technology safely and effectively.
Their role supports multidisciplinary teams in making timely, informed decisions, ultimately leading to improved care outcomes.

Empowering safer maternity care with Radar Healthcare
Delivering safe, high-quality maternity care is a complex challenge—one that demands not only clinical excellence but also robust systems for managing risk, quality, and compliance. Radar Healthcare’s technology is designed to meet this need head-on.
By integrating incident management, risk registers, and real-time analytics into a single platform, healthcare providers can streamline their efforts, reduce administrative burden, and focus on what matters most: delivering exceptional care to patients and families.
Rhian Bulmer, Chief Customer Officer, Radar Healthcare - "Incident management tools not only reduce the burden on healthcare staff but also improve the quality of care by ensuring that incidents are properly documented and analysed. This contributes to a culture of continuous learning and quality improvement in maternity services."

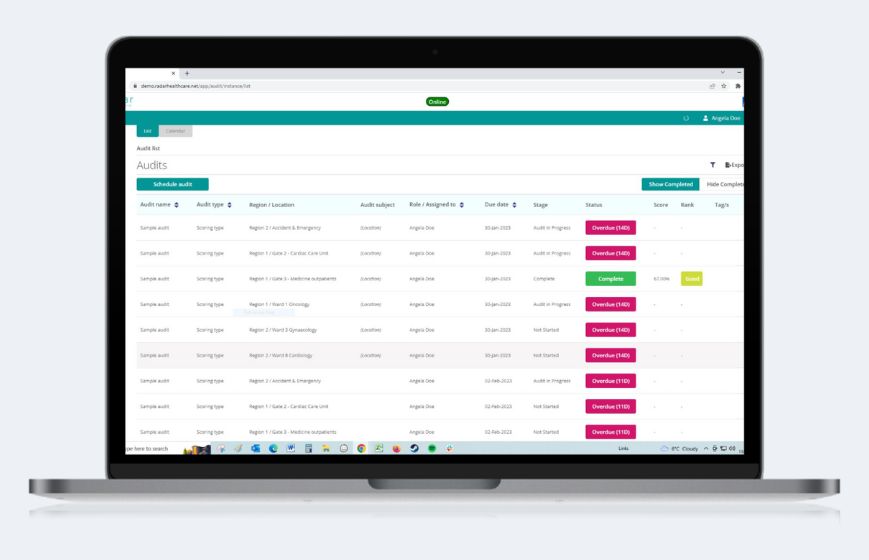
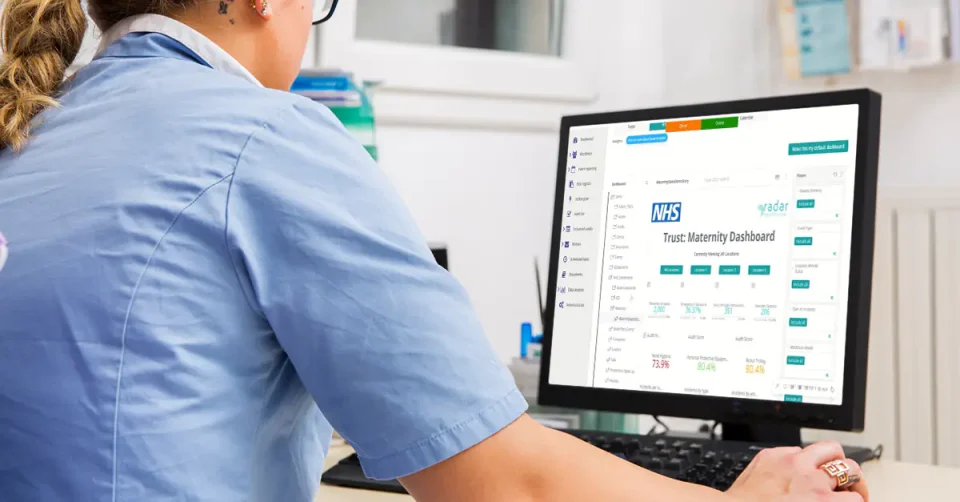
Radar Healthcare’s maternity dashboards offer a comprehensive view of safety and quality metrics, enabling teams to monitor trends, track incidents, and audit performance with precision. These dashboards provide granular insights that support informed decision-making and allow healthcare leaders to respond proactively to emerging risks.
This level of visibility is essential, not just for internal improvement but also for presenting clear, actionable data to regulatory bodies and stakeholders.
Effective risk management is about more than reacting to incidents. It’s about preventing them. Radar Healthcare enables organisations to build tailored risk registers and action plans that address specific challenges in maternity care. This proactive approach helps avoid costly consequences and supports safer, more resilient services by balancing safety with the benefits of personalised care.
Importantly, Radar Healthcare also facilitates direct feedback collection, including both compliments and complaints, from staff and patients, ensuring that frontline voices are heard and acted upon. This feedback loop strengthens engagement, builds trust, and drives meaningful change from the ground up. Clear guidance supports staff in acting quickly on feedback, while actions are regularly reviewed to ensure progress is made.
Improving maternity care requires more than just data; it demands collaboration, transparency, and a commitment to learning from every experience.
At Radar Healthcare, we’re proud to support organisations in building safer, more responsive services through technology that listens, learns, and adapts to the needs of every pregnant woman, baby, and family — including those with a disability or additional care needs.
A vision for the future
The challenges facing maternity care in the NHS are clear. Rising complaints, widening inequalities, safety concerns, and increasing costs all point to a system under pressure. Yet alongside these issues, there are signs of progress.
Dedicated staff, growing use of digital tools, stronger regulatory oversight, and the increasingly influential voices of patients and families are helping to shape a more responsive and accountable maternity service. These developments offer a foundation for meaningful and lasting improvement.
At Radar Healthcare, we believe that by combining technological innovation with compassionate, human-led care, we can ensure that maternity services are not only safe and equitable but also deeply responsive to the needs and experiences of those they serve.
Listening to those voices, whether through feedback, incident reporting, or shared learning, is essential to driving meaningful change.
Our commitment goes beyond technology. We work in partnership with providers and communities to turn insight into action, supporting a culture where learning is continuous, risks are visible and managed proactively, and best practices are shared across teams and organisations.
The future of maternity care can be shaped not by risk alone, but by resilience, safety, and a shared commitment to improvement.